




Why The Ova Care Is Trusted as the Best Fertility and Maternity Hospital

Personalized Support

High Success Rate

24/7 Availablity

5000+ Successful Pregnancies

16+ Years of Experienced Experts

Affordable & Ethical Treatment
Laparoscopic Surgery Hospital in Thane
Laparoscopic gynecological surgery is a minimally invasive surgical method used to diagnose and treat several women’s health conditions through small cuts rather than a large abdominal incision. It is also called keyhole surgery, minimal access surgery, or advanced laparoscopy. At Ova Fertility & Women Care, laparoscopic surgical care in Thane is offered for selected gynecological and pelvic conditions where small-incision surgery can provide accurate diagnosis, precise treatment, reduced tissue trauma, and faster recovery compared with traditional open surgery.
A laparoscope is a thin telescope-like camera inserted through a small incision, usually near the navel. Carbon dioxide gas is used to gently lift the abdominal wall, allowing the surgeon to see the uterus, ovaries, fallopian tubes, pelvis, adhesions, cysts, fibroids, and other pelvic structures on a monitor. Fine instruments may be inserted through additional small cuts when treatment is required.
Laparoscopy is not the right choice for every condition. Some women need only medicines or observation. Some need hysteroscopic treatment, robotic surgery, or open surgery depending on the diagnosis. A responsible laparoscopic surgery hospital in Thane should recommend the technique only when it adds clear value for safety, diagnosis, recovery, or surgical precision.

What Is Laparoscopic Gynecological Surgery?
Laparoscopic gynecological surgery is a modern surgical technique that allows the doctor to view and operate inside the pelvis with small incisions. Instead of opening the abdomen widely, the surgeon uses a camera and fine instruments to perform diagnostic or operative procedures.
Diagnostic laparoscopy is used to inspect the pelvis and identify causes of symptoms such as pelvic pain, suspected endometriosis, unexplained pelvic disease, tubal problems, adhesions, or ovarian pathology. Operative laparoscopy is used to treat selected problems during the same sitting, such as ovarian cysts, endometriosis, adhesions, fibroids, ectopic pregnancy, hydrosalpinx, or other pelvic conditions.
This method is especially valuable in gynecology because many pelvic organs are delicate and closely placed. The uterus, ovaries, tubes, bowel, bladder, ureters, and blood vessels lie near one another. Magnified laparoscopic vision helps the surgeon identify anatomy more clearly and operate with controlled movements.
Laparoscopic Surgery in Thane: When Is It Advised?
A gynecologist may advise laparoscopic surgery when symptoms, examination, ultrasound, blood tests, or previous treatment history suggest a pelvic condition that needs direct assessment or treatment. Common reasons include persistent pelvic pain, painful periods, suspected endometriosis, ovarian cysts, fibroids, adhesions, tubal disease, ectopic pregnancy, chronic lower abdominal pain, pelvic infection history, or abnormal pelvic findings.
Laparoscopy may also be advised when imaging gives incomplete information. Ultrasound is useful, but it may not always show fine adhesions, early endometriosis, mild tubal damage, or the full extent of pelvic scarring. Laparoscopy allows the surgeon to see the pelvis directly and decide whether treatment is needed.
The decision is individualized. At Ova, the doctor reviews symptoms, age, medical history, previous surgeries, scan findings, reproductive goals, anemia, pain severity, and surgical fitness before recommending keyhole surgery in Thane.

Diagnostic Laparoscopy
Diagnostic laparoscopy is performed when the doctor needs to see inside the pelvis to confirm or rule out disease. It may help identify endometriosis, adhesions, ovarian cysts, tubal blockage, hydrosalpinx, pelvic infection-related scarring, fibroids affecting pelvic anatomy, or unexpected pelvic pathology.
During diagnostic laparoscopy, the surgeon may inspect the uterus, ovaries, tubes, pelvic sidewalls, pouch of Douglas, and surrounding structures. A dye test may be performed in selected cases to assess whether the fallopian tubes are open. This can be useful when previous tubal tests are uncertain or when pelvic disease is suspected.
Diagnostic laparoscopy often provides clarity after months of symptoms or inconclusive reports. If a treatable condition is found and consent has been taken, operative correction may sometimes be done during the same procedure.
Operative Laparoscopy
Operative laparoscopy is used to treat selected gynecological conditions through small incisions. Depending on the diagnosis, the surgeon may remove ovarian cysts, release adhesions, treat endometriosis, remove selected fibroids, manage ectopic pregnancy, correct tubal pathology, drain or remove diseased tissue, or perform hysterectomy when medically appropriate.
Operative laparoscopy requires surgical skill because the surgeon works with long instruments while watching the operative field on a monitor. The technique demands careful handling of tissues, control of bleeding, safe use of energy devices, and awareness of nearby organs.
At Ova, operative laparoscopy is planned with safety, symptom relief, and reproductive health in mind. Surgery is not recommended simply because a condition is visible. It is advised when the expected benefit is meaningful.
Laparoscopic Pelvic Surgery
Laparoscopic pelvic surgery may be useful for pelvic pain, adhesions, endometriosis, ovarian cysts, fibroids, hydrosalpinx, and other pelvic conditions. Pelvic disease can distort normal anatomy. Adhesions may pull the ovaries or tubes out of position. Endometriosis may cause inflammation, scarring, and cysts. Large cysts or fibroids may press on surrounding organs.
The laparoscopic route allows the surgeon to inspect the pelvis carefully and treat selected findings with minimal access. This can reduce the need for larger incisions in suitable cases. However, severe disease, dense bowel adhesions, very large masses, suspected malignancy, or unstable medical condition may require another surgical approach.
A skilled surgeon must know when laparoscopy is beneficial and when it is safer to change the plan.
Laparoscopic Reproductive Surgery
Laparoscopic reproductive surgery focuses on preserving reproductive organs and function whenever possible. It may include treatment of endometriosis, ovarian cysts, adhesions, tubal disease, hydrosalpinx, or fibroids that affect pelvic anatomy. This type of surgery requires special care because excessive removal of healthy ovarian tissue or aggressive handling of pelvic organs can affect future reproductive potential.
For ovarian cysts, the aim is to remove the cyst wall while preserving healthy ovarian tissue. For endometriosis, the goal is to treat disease while protecting ovarian reserve and surrounding organs. For adhesions, the surgeon releases scar tissue carefully to restore pelvic anatomy where possible. For tubal disease, the decision depends on whether the tube can function after correction.
Fertility-preserving surgery is not only about doing the operation. It is about choosing the correct operation, using gentle technique, and planning the next step after recovery.
Laparoscopic Adhesiolysis
Adhesions are bands of scar tissue that can form after infection, surgery, endometriosis, inflammation, or pelvic disease. Pelvic pain may occur, organ movements may be restricted, the tubes may be distorted, bowel discomfort may occur, or difficulties with conception may occur.
Laparoscopic adhesiolysis means releasing adhesions through keyhole surgery. The procedure can help restore anatomy in selected cases, but adhesions may recur. The surgeon must avoid unnecessary trauma because further tissue injury can create new adhesions.
Before advising adhesiolysis, the doctor considers symptoms, disease severity, previous surgeries, bowel involvement, and expected benefit. Not every adhesion requires treatment. The decision must be clinically justified.
Laparoscopic Ovarian Surgery
Laparoscopic ovarian surgery may be used for selected ovarian cysts such as simple cysts, endometriotic cysts, dermoid cysts, persistent cysts, painful cysts, or cysts with concerning features that require removal. The goal is safe treatment while preserving ovarian function as much as possible.
Ovarian surgery must be planned carefully. Removing too much normal ovarian tissue can affect ovarian reserve. This is especially important for women with previous ovarian surgery, endometriosis, low ovarian reserve, or future reproductive goals. The surgeon should explain whether observation, medicine, repeat scan, laparoscopy, or open surgery is most suitable.
Sudden severe pelvic pain with vomiting may suggest torsion or rupture and needs urgent medical attention.
Laparoscopic Tubal Surgery
The fallopian tubes are important in natural conception because they pick up the egg and provide the site where fertilization usually occurs. Tubal problems may include blockage, hydrosalpinx, adhesions, infection-related damage, ectopic pregnancy, or previous surgery-related scarring.
Laparoscopic tubal surgery may include assessment of tubal patency, treatment of adhesions around the tubes, management of hydrosalpinx, or treatment of ectopic pregnancy. A methylene blue dye test may be used in selected cases to assess tubal openness.
Not every blocked or damaged tube can be repaired usefully. Sometimes a tube may be open but not function well. The doctor explains whether tubal correction is likely to help or whether another plan is safer.
Endometriosis and Laparoscopy
Endometriosis is a common reason for laparoscopic gynecology consultation. It can cause severe period pain, chronic pelvic pain, painful intercourse, bowel or bladder discomfort during periods, ovarian chocolate cysts, adhesions, and distorted pelvic anatomy.
Laparoscopy can help diagnose and treat endometriosis in selected patients. Visible disease may be excised or treated, adhesions may be released, and ovarian endometriotic cysts may be managed when clinically indicated. The extent of surgery depends on age, symptoms, cyst size, organ involvement, previous surgeries, and reproductive plans.
Endometriosis surgery must be precise and conservative where needed. Aggressive surgery can sometimes harm ovarian reserve or surrounding organs. A balanced plan protects long-term health.
Fibroids and Laparoscopic Surgery
Fibroids are non-cancerous growths of the uterus. Some cause no symptoms and only need monitoring. Others may cause heavy bleeding, anemia, pelvic pressure, pain, frequent urination, constipation, or reproductive concerns.
Laparoscopic fibroid removal may be considered when fibroids are suitable in size, number, and location. Larger or multiple fibroids may require advanced skill or another approach. When it comes to preserving the uterus, it is critical to perform a secure uterine repair.
In some women, hysterectomy may be advised if symptoms are severe, family is complete, and other treatments are unsuitable. The decision should be based on symptoms, age, anemia, scan findings, and patient preference after counselling.
Laparoscopic Hysterectomy
Laparoscopic hysterectomy means removal of the uterus through minimally invasive surgery. It may be advised for selected women with heavy bleeding, fibroids, adenomyosis, prolapse, chronic pain, or other conditions where removing the uterus is medically appropriate.
Hysterectomy is not the first treatment for every menstrual or pelvic problem. The doctor should review medical treatment, hormonal options, minor procedures, and organ-preserving alternatives where suitable. If hysterectomy is advised, the patient should understand whether the ovaries will be preserved, what recovery will involve, and how the procedure may affect future health.
Laparoscopic hysterectomy can offer smaller scars, less pain, shorter stay, and faster recovery in suitable patients compared with open surgery.
Laparoscopy Versus Open Surgery
Open surgery requires a larger incision and gives direct access to the pelvic organs. It may still be necessary for very large masses, suspected cancer, severe adhesions, emergency bleeding, or cases where safe laparoscopic access is not possible.
Laparoscopic surgery uses small incisions, a camera, and fine instruments. In suitable cases, it can reduce pain, blood loss, infection risk, scarring, hospital stay, and recovery time. Many simple laparoscopic procedures may allow discharge the same day or after short observation, depending on the procedure and patient condition.
The best method depends on diagnosis and safety. A modern surgical team should be skilled in minimally invasive surgery but willing to choose open surgery when it is safer.
Laparoscopy Versus Robotic Surgery
Both laparoscopy and robotic surgery are minimally invasive techniques. Laparoscopy uses straight instruments controlled directly by the surgeon at the operating table. Robotic surgery uses robotic arms controlled by the surgeon from a console, with wristed instruments and magnified 3D visualization.
Laparoscopy is highly effective for many gynecological procedures. Robotic surgery may help in selected complex cases requiring advanced suturing, difficult pelvic access, or fine dissection. The choice depends on disease complexity, surgeon expertise, patient anatomy, cost, and expected benefit.
This page focuses on laparoscopic gynecological surgery. Robotic surgery should be discussed separately when relevant.
Benefits of Laparoscopic Surgery
In suitable patients, laparoscopic surgery may provide smaller cuts, less pain, lower wound infection risk, shorter hospital stay, faster recovery, earlier movement, less scarring, and quicker return to routine activities compared with open surgery. Your current page correctly explains that some simple laparoscopic procedures may allow patients to go home the same evening, while traditional surgery may need longer recovery.
Laparoscopy also offers diagnostic benefits. The surgeon can directly see the uterus, ovaries, tubes, adhesions, endometriosis, cysts, fibroids, and pelvic anatomy. This can be valuable when symptoms are persistent but routine tests do not explain the cause.
These benefits depend on correct case selection, surgical skill, patient health, and the complexity of the operation.
Risks and Limitations
Laparoscopic surgery is generally safe in trained hands, but it is still surgery. Possible risks include bleeding, infection, anesthesia complications, injury to bowel, bladder, ureter, blood vessels or uterus, gas-related shoulder pain, urinary problems, blood clots, wound issues, delayed recovery, adhesions, or conversion to open surgery.
Some patients have higher surgical risk due to previous abdominal operations, severe endometriosis, dense adhesions, obesity, pelvic infection, bowel disease, heart disease, lung disease, or uncontrolled medical conditions. These factors must be discussed during pre-surgical assessment.
Laparoscopy may not be suitable if the mass is very large, malignancy is suspected, the patient is unstable, or the disease cannot be safely managed through keyhole access. Honest counselling is essential.
What Happens During the Procedure?
Most laparoscopic gynecological surgeries are performed under general anesthesia. After anesthesia, the abdomen is cleaned and small incisions are made. Carbon dioxide gas is introduced to create working space. A laparoscope is inserted, and the pelvic organs are examined. Additional small ports may be placed for instruments if treatment is planned.
The surgeon performs the required procedure, controls bleeding, removes tissue if needed, and checks the pelvis before completing the surgery. We remove the instruments, release the gas, and close the small incisions.
The patient is shifted to recovery, where pulse, blood pressure, breathing, pain, bleeding, urine output, and alertness are monitored.
Recovery After Laparoscopic Surgery
Recovery depends on the type of procedure. Some patients may go home the same day, while others may need overnight or longer observation. Mild abdominal pain, shoulder-tip pain from gas, bloating, nausea, tiredness, and small wound discomfort are common in the first few days.
Walking is usually encouraged early. Heavy lifting, intense exercise, intercourse, and long travel should be avoided until the doctor allows. Wound care instructions, medicines, diet, bathing, and follow-up visits are explained before discharge.
Return to work depends on the surgery and job type. Simple diagnostic procedures may need less recovery time, while cyst removal, fibroid surgery, endometriosis surgery, or hysterectomy may need longer rest.
Warning Signs After Surgery
Contact the doctor urgently if you have fever, worsening abdominal pain, persistent vomiting, heavy bleeding, foul discharge, wound redness or pus, severe bloating, difficulty passing urine, fainting, breathlessness, chest pain, calf swelling, or severe shoulder pain that does not improve.
Early reporting of symptoms helps prevent complications. Do not ignore severe pain or fever after surgery.
Pre-Surgery Checklist
Before laparoscopic surgery, carry ultrasound reports, MRI if done, blood tests, Pap smear or biopsy reports if relevant, previous surgery notes, discharge summaries, current medicines, allergy details, and medical-condition records. Tell the doctor if you take blood thinners, diabetes medicines, blood pressure tablets, thyroid medicines, or hormonal treatment.
Pre-surgery evaluation may include blood tests, urine tests, ECG, anesthesia fitness, imaging review, and medical specialist opinion when required. The doctor explains fasting instructions, admission timing, expected hospital stay, procedure plan, risks, alternatives, and consent.
A well-prepared patient has fewer surprises and better recovery confidence.
Why Choose Ova for Laparoscopic Surgery in Thane?
Ova Fertility & Women Care provides laparoscopic surgery in Thane for selected gynecological, pelvic, and reproductive health conditions. The current Ova page already highlights keyhole surgery, reduced post-surgery pain, lower infection chances, same-day discharge for selected simple procedures, diagnostic value in pelvic assessment, tubal evaluation, ovarian visualization, endometriosis diagnosis, chocolate cyst removal, fibroid removal, hysterectomy, and complex laparoscopy requiring advanced expertise. This rewrite strengthens that foundation with clearer patient education and decision support.
Ova Care is located at 1st Floor, Tieten Medicity Hospital, Kasarvadavali, Ghodbunder Road, Thane West. Patients from Kasarvadavali, Ghodbunder Road, Manpada, Waghbil, Hiranandani Estate, Kolshet, Majiwada, Vasant Vihar, Pokhran Road, Kalwa, Mulund, Airoli, Dombivli, and nearby areas can consult for minimally invasive gynecological surgery and keyhole procedures.
Gynaecology & Endoscopy
Let's Meet Up
contact
Frequently Asked Questions
It is minimally invasive gynecological surgery performed through small incisions using a camera and fine instruments to diagnose or treat pelvic conditions.
No. Laparoscopy is keyhole surgery. A laser is not always used. The term “laser surgery” is often used casually but is not technically the same.
It may treat selected ovarian cysts, endometriosis, adhesions, fibroids, ectopic pregnancy, hydrosalpinx, pelvic pain causes, and hysterectomy cases.
Pain is usually less than open surgery, but some discomfort, bloating, and shoulder pain from gas may occur. Pain medicines are given after surgery.
Simple procedures may allow same-day discharge or short observation. More complex surgery may require longer stay depending on the operation and recovery.
Yes. Diagnostic laparoscopy can identify endometriosis, adhesions, cysts, pelvic infection-related scarring, and other causes that may not be clear on routine tests.
Scars are usually small because the incisions are small. The healing process depends on the type of skin, wound care, and details of the procedure.
In selected cases, laparoscopy can support fertility-preserving treatment by managing cysts, adhesions, endometriosis, or tubal disease while protecting reproductive organs.
Risks include bleeding, infection, anesthesia complications, organ injury, blood clots, urinary issues, and rare conversion to open surgery.
A gynecologist will review your symptoms, reports, examination, medical history, and treatment goals before advising whether laparoscopy is suitable.
Related Searches:
Intrauterine Insemination (IUI) Treatment in Thane, Pre-Implantation Genetic Testing in Thane, Blastocyst Culture And Transfer Clinic in Thane, Laser Assisted Hatching Treatment in Thane, Egg/Sperm/Embryo Cryopreservation Freezing, Endoscopy In Fertility Treatments, Pregnancy Care, Birthing, Ultrasound In Pregnancy, High Risk Pregnancy Treatment Care With ICU Facility, Laparoscopic Surgery, Hysteroscopic Surgery, Menopause, Puberty Adolescence Treatment, Oncofertility,Male Infertility Treatment in Thane, best ivf hospital, ivf specialist, ivf doctor in thane, fertility treatment in thane, dr. snehal kohale ivf specialist
Our Latest Articles

Laser Assisted Hatching Treatment | IVF Procedure & Benefits
Laser Assisted Hatching Treatment: IVF Procedure, Benefits & Who May Need It Laser assisted hatching is an advanced IVF technique used to support embryo implantation in selected fertility cases. During IVF, an embryo has to “hatch” from its outer covering before it can attach to the uterine lining. In some
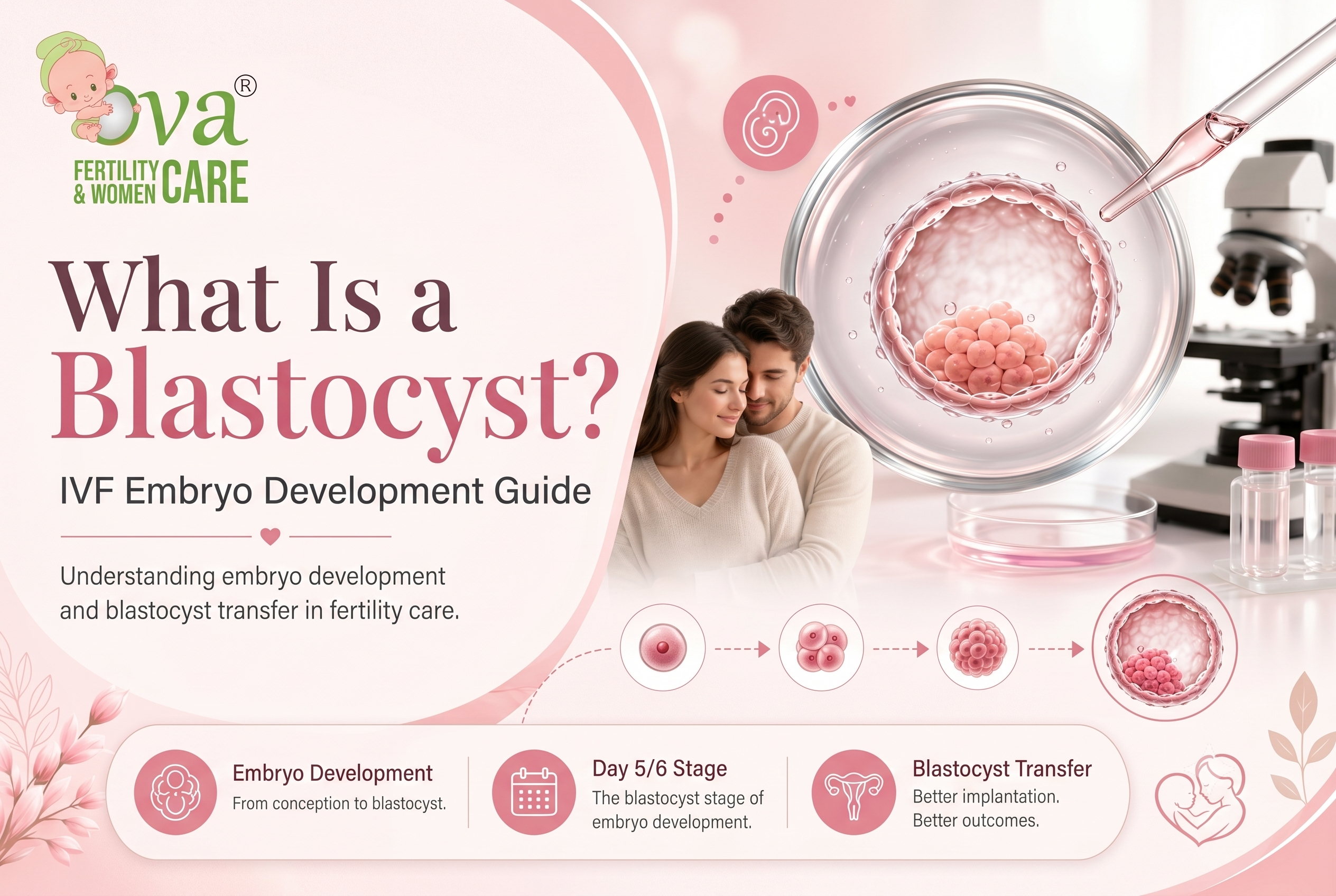
What Is a Blastocyst? | IVF Embryo Development Guide
What Is a Blastocyst? IVF Embryo Development & Blastocyst Transfer Guide What is a blastocyst? This is one of the most common questions couples ask during IVF treatment, especially when the doctor talks about embryo development, embryo grading, blastocyst culture, or blastocyst transfer. In simple words, a blastocyst is an
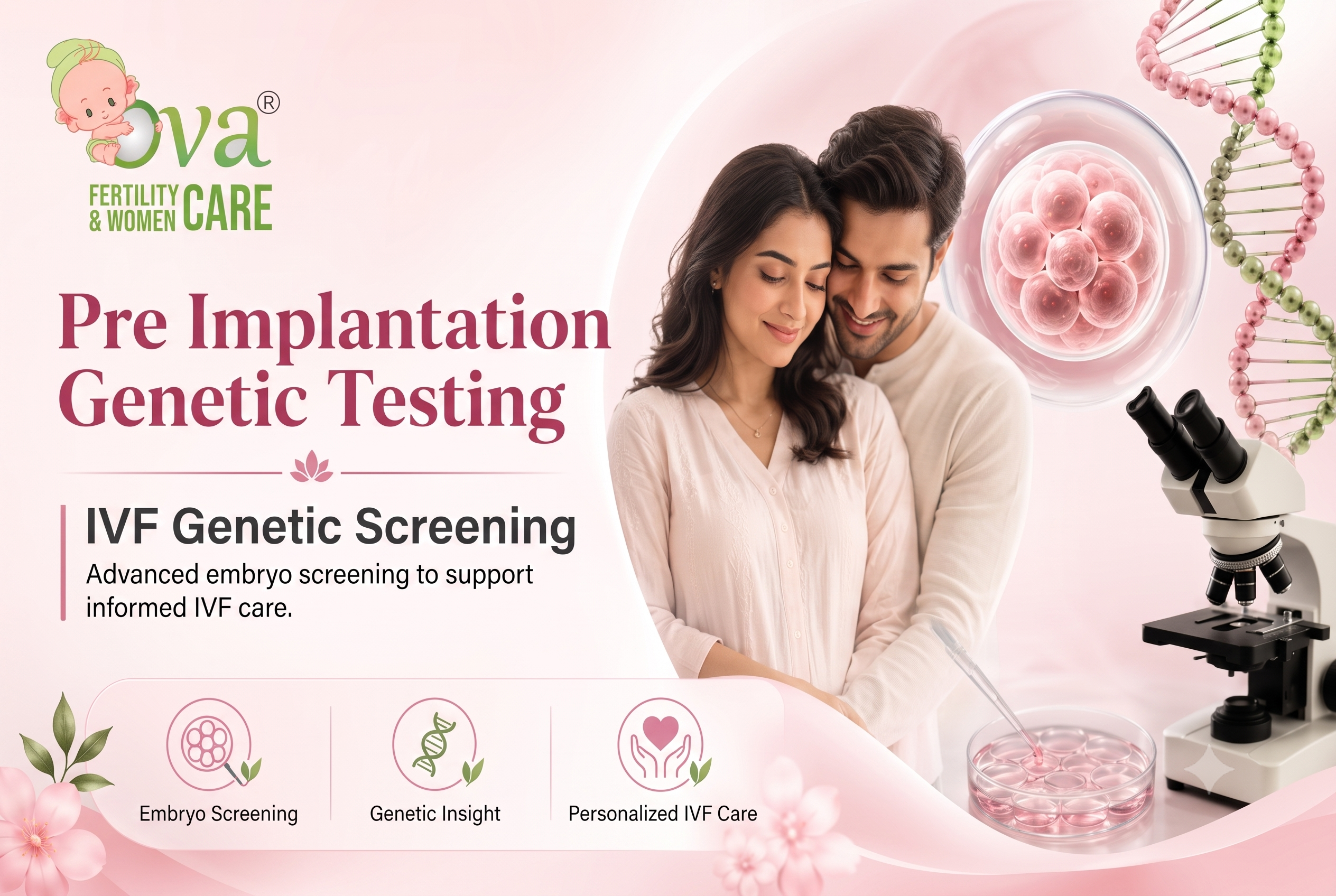
Pre Implantation Genetic Testing | IVF Genetic Screening
Pre Implantation Genetic Testing: IVF Genetic Screening for Healthier Embryo Selection Pre implantation genetic testing is an advanced fertility procedure used during IVF to check embryos for certain genetic or chromosomal abnormalities before embryo transfer. For many couples, IVF is not just a treatment. It is an emotional journey filled
 No need to worry, your data is 100% Safe with us!
No need to worry, your data is 100% Safe with us!